
I read a study (in a reputable journal) this week, with the title, “Video Telemedicine Experiences In COVID-19 Were Positive, But Physicians And Patients Prefer In-Person Care For The Future.” Of course, this caught my eye. My experience has been different. Patients consistently tell me how much they enjoy the convenience of receiving care via telehealth. I fully admit this is anecdotal and subject to all the potential biases anecdotal observations are subject to, but I do believe this to be the case. Likewise, over the years, other studies (innumerable, really) have shown high patient satisfaction with telehealth. Those caveats aside, this headline and some of the study findings give pause for thought.
I don’t know anyone who disagrees that the ideal emotional connection results from a rich sensory experience, often occurring in person. However, we’ve long assumed that patients will trade this rich sensory experience for the convenience of receiving care in their homes.
The authors of the article linked above surmise that most of the preferences toward in-person care pivot around the notion that video telehealth omits any physical examination. The doctors they surveyed seemed quite focused on this challenge. Patients may be more forgiving, but the other undercurrent from this paper was that, somehow, telehealth visits are of lesser quality.

I also ran across this study from the dermatology literature, stating that 48.5% of patients surveyed in Singapore felt that their teledermatology experience was substandard. So, this is not a one-off and you may have read other similar reports. As telehealth makes its post-pandemic effort to be seated at the grownup table, I’d argue that we must address this issue of competing with in-person care.
How do we do that?
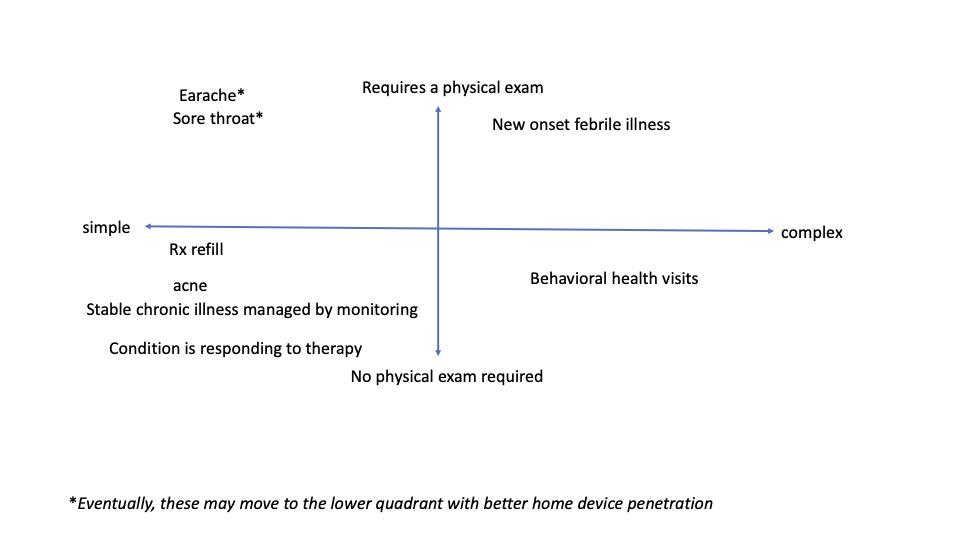
Let’s start with the physical exam issue. I and others have repeatedly made the case that not all healthcare decisions made by a practitioner require data from a physical examination. For those that do, there are exciting home-based technologies that can enrich the data coming from the patient to aid in that decision-making. One example is the Tytocare device which allows the practitioner to do ear and throat exams, listen to the heart, and take a temperature. While this device, and others like it, are not in wide distribution yet, the time when we have easy access to this type of tool is around the corner. In the meantime, I implore my clinical colleagues to educate their staff to identify those presenting complaints that will likely require a physical exam, so those patients can be triaged directly to an in-person setting.
Another variable to consider is complexity. Sometimes when patients need us, it is for something very simple – a prescription refill, a quick follow-up to assure us they are responding to therapy, or a chronic condition check-in where the discussion is about some home data they have been collecting (e.g., blood glucose or blood pressure). For patients with a simple issue like this (better still, with whom you have a preexisting relationship), telehealth is a win for both parties.
By the way, an ongoing relationship with a behavioral health therapist matches these criteria to a T, probably accounting for behavioral telehealth’s rising popularity and success.
I have started a diagram to help visualize these issues.
After we put aside the provider decisions that do not require a physical exam, and cordon off the simple, routine care decisions (often but not always involving a preexisting relationship), what is left? Should we leave it at that and say telehealth is good for these use cases, but the rest are better in-person?
I would argue that this gives innovators their roadmap and a call to action:
- Create more interactive technologies and make it feel like two participants are in the same physical space. For a time during the last decade, some of the tech giants had room videoconferencing systems that were set up as mirror images of one another, so participants felt like they were around a table in the same room. These were prohibitively expensive for widespread use, but with the emergence of virtual reality and augmented reality, it is not hard to imagine we could make the experience much more “up close and personal” without too much of an added cost burden.
- Figure out how to get technologies like the Tytocare into every medicine cabinet. At some point in history, we did this with the mercury thermometer. Perhaps, we can learn from history how that was accomplished.
- There are other technologies that will enhance a clinician’s decision-making ability when the patient is not in the same room. Home lab tests (e.g., Everlywell) and digital biomarkers are two examples.
So how do we create the right tools, a comfortable, convenient virtual environment, and a clinical workflow that identifies when and which patients and conditions are appropriate for telehealth services?
When we figure those things out – and, of course, reimbursement of virtual care services – we will have a modality of care that will eliminate the need to compete with in-person care. It will enhance and complement the care that our patients receive in hospitals and doctors’ offices, and we can focus our significant energies on creating an omnichannel care system. Isn’t that really our goal?