
I recently gave a talk to a group of primary care clinicians updating them on the state of telehealth. My take-home message was: “This is a mature care delivery model now. You should decide how much you want to integrate it into your practice.”
That got me thinking about why telehealth has not become more of an imperative, rather than remaining an option.
Yes, we went through the pandemic, and that raised awareness about virtual care among our patients. With rare exception, the preferred delivery platform for behavioral health is now telehealth. Any number of companies (e.g., Amwell, Teladoc, MDLIVE) have made a successful business delivering telehealth through health plans and large employers. Another group of companies (e.g., Ro, HIMS, MeMD) are thriving with direct-to-consumer, pay cash services.
However, we are still underperforming as an industry compared to the promises made and the vision we’ve spun, especially in the case of traditional healthcare providers. Why is that, and more pointedly, why is telehealth still an option instead of an imperative?
It’s not as if we haven’t tried to use every lever we could think of to accelerate adoption. Indulge me while I list a few.
- The most consistent argument is telehealth increases access, often coupled with “patients are demanding this.” Extending access is a public health value but not necessarily an individual clinician priority, especially in cases where the clinician has a busy practice to begin with. Keep in mind that we have a significant supply/demand mismatch in health care, so most providers are not focused on extending access.
- A second strategy is to affect reimbursement policy for telehealth. I have been personally involved in this for the past seven years. The effects have been modest. Though we’ve created several reimbursement codes, their implementation has been challenging, and coverage at the individual payer level is inconsistent. In short, the effort to implement a scaled telehealth or hybrid care model is often more costly than the corresponding reimbursement rewards.
- Nature even gave us a pandemic to prove the utility of telehealth. Though our star shone brightly for most of 2020, it has faded somewhat since.
Except for three months or so in 2020, telehealth has remained an option.
So, I ask, “What would it take to make telehealth an imperative?” Are there other examples of care processes that we consider imperative today that weren’t always, and what can we learn from these models to apply to our strategy going forward?
I’ll share one non-technology example to illustrate the mental exercise. Before Semmelweis made the association between handwashing and improved obstetrical outcomes in 1847, the idea of a clinician cleaning one’s hands between patients was nonexistent. Sadly, Semmelweis was ahead of his time. Pasteur published the germ theory of disease in 1861. Simmelweis died destitute. But…imagine a world where we, as clinicians, don’t wash hands between patients. Further, consider the additional cost to hospitals and care providers for cleansers, dispensers, glovers, sterile drapes, etc. Today, if you visited a doctor who tried to do surgery on you or deliver a baby without hand hygiene, you’d exit the building as fast as you could. Hand hygiene is an imperative!
Another example that may be a better analogy is minimally invasive surgery (MIS).
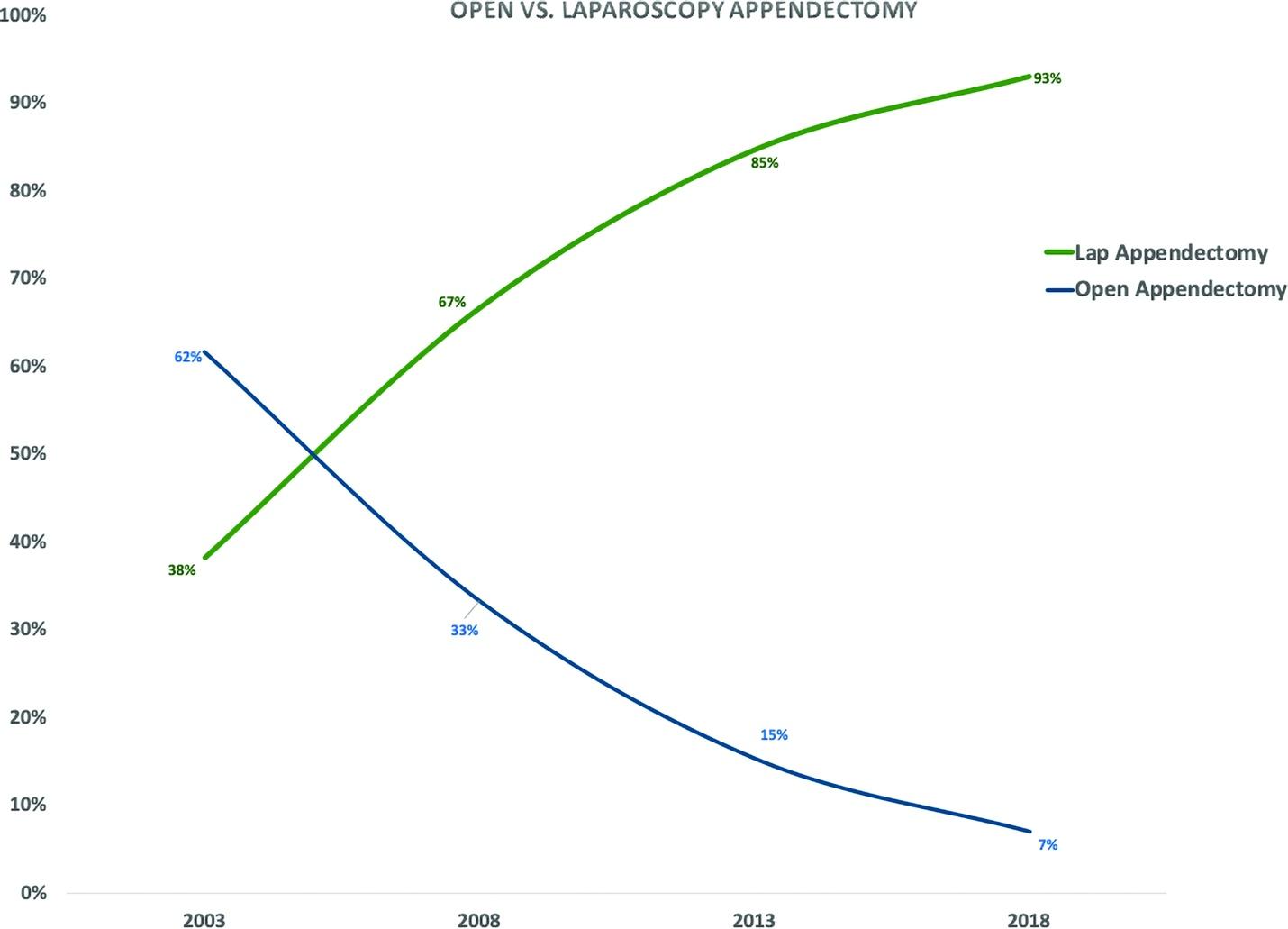
This figure (from https://doi.org/10.4293/JSLS.2020.00076) shows the change in the adoption of laparoscopic appendectomy compared to open appendectomy from 2003-2018. Such a dramatic change in the span of only 15 years. Another data point: 96% of all gall bladder operations are now done through a laparoscope. MIS is imperative now compared to 20 years ago. How did we get there, and can we apply any of that history – and trajectory – to telehealth adoption?
After studying the adoption of MIS and consulting with a surgeon* who lived through this change, I came up with five characteristics of MIS that sped its adoption.
Patient Benefits: MIS procedures generally offer quicker recovery times, less pain, and smaller scars compared to traditional open surgeries. This translates to a shorter hospital stay, reduced risk of infection, and a faster return to normal activities for patients. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5443851/.
Surgeon Advantages: Minimally invasive techniques often provide surgeons with better surgical field visualization through laparoscopes or other specialized instruments. This can lead to greater precision and control during the procedure.
Shifting Surgical Philosophy: Over time, the medical field has moved towards a less invasive approach whenever possible. MIS aligns with this philosophy by minimizing trauma to the patient’s body.
Positive Clinical Outcomes: As research demonstrated the effectiveness and safety of MIS compared to traditional open surgery for various procedures, surgeons became more confident in adopting these techniques. https://pubmed.ncbi.nlm.nih.gov/12791133/.
Technological Advancements: The development of sophisticated tools and equipment like laparoscopes, robotic arms, and advanced imaging techniques significantly aided the adoption of MIS. These advancements improved both the efficiency and safety of minimally invasive procedures. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3117518/.
Some interesting insights emerge as I look for parallels from MIS to telehealth.

- Patient benefits are a key driver for both. Plenty of data shows that patients adopt telehealth for convenience and ease of access. One difference seems to be that they don’t demand telehealth. However, they expect MIS. Is this a matter of time? Does it relate to the fact that surgery is invasive and diagnostic/therapeutic services are not? An office visit interrupts your day; open surgery can impact weeks or more of your life.
- One crucial difference may be that MIS has advantages for the surgeon, whereas implementing telehealth is often seen as an additional burden to the practitioner.
- There has yet to be a shift in thinking about how medical care is provided that corresponds to the shifting surgical philosophy noted above.
- An objective observer would also say that the data on positive clinical outcomes is not as strong for telehealth as for MIS.
- While both are rooted in technological advancements, there is a sense that the tech innovations leading the way for MIS are a positive force for humanity. In contrast, the use of technology in telehealth is possibly seen as compromising the quality of care.
As telehealth evangelists, can we create a strategy or roadmap for adoption based on these insights? I found the comparison helpful in clarifying my thinking and offer the following suggestions.
- We need patients to be more vocal and opinionated on their preference for telehealth, even making provider choices based on that.
Need: Patient education and patient advocates
- We must double down on the evidence we collect and publish regarding quality and outcomes. That would help with three and four above.
Need: a robust research agenda, including data repositories, research awards and appropriate funding
- We should redouble efforts to make it seamless for practitioners to adopt telehealth. Many friction points (beyond the scope of this piece) still exist.
Need: create the need for telehealth by addressing clinicians’ pain points
- We should work on making the technology supporting telehealth better than in-person and dispel the negative image of poor care quality.
Need: design patient/clinician-centric tech and educate consumers/patients to build their confidence in telehealth and effectively engage in virtual interactions with clinicians
Can we apply these insights to sharpen our strategy in the spirt of achieving the right level of telehealth adoption? Let me know what you think.
*a special thanks to Dr. Andrew Watson, who gave critical feedback during the creative process.